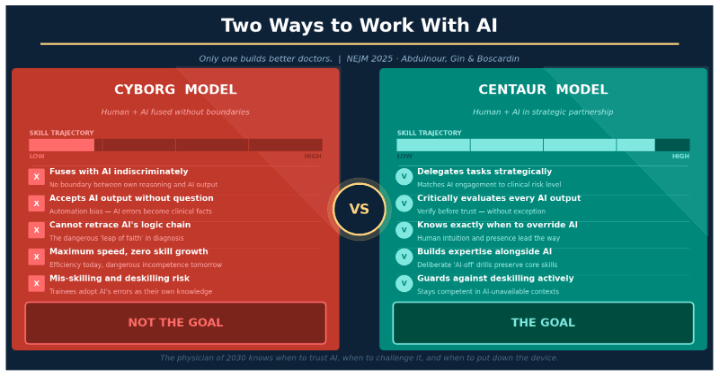
Cyborg and centaur describe two different ways a person can work with AI: a cyborg blends so tightly with the AI that the human and the tool function as one process, while a centaur keeps a firm boundary, strategically delegating specific subtasks to AI while retaining control of judgment and final decisions.
New 2026 cross-industry research has added a third mode, the self-automator, who hands an entire task to AI with minimal oversight, and found that centaurs consistently produce the most accurate outcomes. For clinical training, where errors carry real consequences, that finding matters more than it might in most other fields.
Where does the cyborg-centaur framework come from?
The NEJM's 2025 supervisory framework for clinical AI use introduced cyborg and centaur as the two poles of human-AI collaboration. A cyborg represents tight, largely indiscriminate fusion with AI — maximum efficiency, minimal independent growth, and real risk if the AI is wrong. A centaur represents strategic delegation: using AI deliberately for the tasks it's genuinely good at, while keeping critical evaluation, judgment, and final decision-making firmly with the human. The NEJM's framing was unambiguous about which one medical training should aim for.
What's new in the research?
A widely discussed cross-industry study out of MIT Sloan, Harvard Business School, and collaborating researchers , covered by Fortune and MIT Sloan Management Review in early 2026, tracked how knowledge workers actually used generative AI on real tasks and found three distinct patterns, not two. Cyborgs blended continuously with AI throughout a task. Centaurs (about 14% of the studied population) practiced what the researchers call "directed knowledge co-creation" using AI for specific subtasks like mapping a problem or refining a draft, while staying in the driver's seat throughout. Self-automators (about 27%) engaged in "abdicated knowledge co-creation", delegating whole workflows to AI with minimal iteration or critical engagement.
The performance data is the part clinical educators should sit with. Centaurs achieved the highest accuracy of the three groups, outperforming both cyborgs and self-automators at getting the right answer, because maintaining control over the process let them catch AI's confident-but-wrong recommendations before those recommendations became the final output. Both cyborgs and centaurs outproduced self-automators on persuasiveness, but only centaurs combined that with reliable accuracy.
Is the cyborg mode actually bad, though?
Here's the more nuanced point this new research adds to the original NEJM framing: cyborgs aren't simply "doing AI wrong." They're building a different kind of skill entirely. The researchers describe cyborgs as developing newskilling (genuine expertise in prompting, iterating, and extracting maximum value from continuous AI interaction), as opposed to the upskilling centaurs experience, where deepening their own domain expertise happens alongside selective AI use. Newskilling is a real skill. It's just not the same skill as clinical judgment, and in medicine, clinical judgment is the one that has to hold up when the AI isn't in the room, in the OR, on a code, at 3 a.m. with no signal.
This connects directly to the never-skilling and false-proficiency research we covered earlier in this series. Self-automator behavior, applied to clinical training, is close to a best-case description of how false proficiency gets built: a trainee who delegates the differential, the note, and the literature search wholesale may look fluent and fast, without ever exercising the reasoning that needs to be load-bearing the day the AI is unavailable or wrong.
What does this look like in a teaching hospital right now?
One of the most disorienting moments in medical education today is what the NEJM calls the "inversion of expertise". For the first time, trainees may be more fluent with a core clinical tool than their supervisors are. I've felt this myself. As a neonatologist, I've spent decades building clinical intuition, pattern recognition that lives in my fingertips, my ears, my gut. A third-year resident who grew up with AI can query a model, synthesize the output, and generate a differential faster than I can type the chief complaint.
Does that make the resident a better clinician? Not yet. The speed of output and quality of judgment are different things, and the research above suggests they can move in opposite directions if the resident is operating as a self-automator rather than a centaur. But it should make every attending a more curious mentor, and it's exactly the inversion that DEFT-AI-style supervision was designed to address: not to slow trainees down, but to make sure the human reasoning checkpoint survives the speed.
How should training programs apply this?
The physician of 2030 isn't someone who out-computes AI. That contest was lost the moment AI could pass a licensing exam. The physician of 2030 is someone who knows when to delegate, when to challenge the output, and when to put the device down and just listen to the patient, in other words, a centaur by habit, not by accident. That habit is teachable: structured prompts requiring an independent differential before AI consultation, debriefs that ask trainees to defend or overturn an AI suggestion, and supervision models like DEFT-AI that build the checkpoint into the workflow rather than hoping trainees develop it on their own.
That's a teachable skill. But only if training programs decide to teach it on purpose, rather than letting each trainee discover their own mode by accident.
How do you actually tell which mode a trainee is in?
In practice, the tell isn't how fast a trainee produces an answer, it's what happens when you ask them to explain it. A self-automator, pressed to defend a differential, will often default back to restating what the AI said, sometimes word for word. A cyborg can usually explain how they got the AI to that answer (which prompts worked, what they iterated on), but may struggle to defend the clinical logic independent of the tool. A centaur can set the AI output aside entirely and rebuild the reasoning from first principles, because they never fully outsourced it in the first place. That one question, "set the AI aside, walk me through your reasoning", is a remarkably cheap diagnostic, and it costs a training program nothing to start asking it on rounds tomorrow.
FREQUENTLY ASKED QUESTIONS
Q: What is the difference between a cyborg and a centaur in AI collaboration?
A: A cyborg blends tightly and continuously with AI throughout a task, with the AI exerting significant control over how the work gets done. A centaur uses AI selectively for specific subtasks while retaining control over judgment, evaluation, and the final decision.
Q: What is a "self-automator"?
A: A self-automator is a 2026 research term for someone who delegates an entire task or workflow to AI with minimal iteration or critical review — the mode researchers found least accurate and most associated with the diminished-reasoning risks described in never-skilling research.
Q: Which mode produces the best results — cyborg, centaur, or self-automator?
A: Cross-industry research found centaurs achieved the highest accuracy of the three modes, because maintaining control over the process let them catch AI errors before they became final output — a finding with direct relevance to clinical decision-making, where errors carry real consequences.
Q: Is being a "cyborg" automatically bad for trainees?
A: Not entirely — cyborgs develop genuine expertise in AI interaction itself, called "newskilling." The concern in clinical training isn't that this skill is worthless, it's that it's a different skill from clinical judgment, and clinical judgment is the one that has to function when AI isn't available.
SOURCES & CITATIONS
• Abdulnour RY, Gin B, Boscardin C. Educational Strategies for Clinical Supervision of Artificial Intelligence Use. N Engl J Med. 2025;393:786-797.
• Cyborgs, Centaurs and Self-Automators: The Three Modes of Human-GenAI Knowledge Work and Their Implications for Skilling and the Future of Expertise. Randazzo, Lifshitz-Assaf, Kellogg, Dell'Acqua, Mollick, Candelon, Lakhani. SSRN / Harvard Business School, 2025.
• 3 ways to use AI: Are you a cyborg, a centaur, or a self-automator? MIT Sloan Management Review, 2026.
• Are you a cyborg, a centaur, or a self-automator? Why businesses need the right kind of "humans in the loop" in AI. Fortune, January 2026.